Microgravity’s hidden tax: what Artemis-era crews are teaching us about the human body
Fresh signals from NASA’s Artemis 2 program—reinforced by observations shared by ESA astronaut Andreas Mogensen and NASA astronaut Jasmin Moghbeli—are sharpening a long-standing truth in space medicine: microgravity doesn’t merely weaken the body; it rewires it. The familiar headlines remain valid—bone demineralization, muscle atrophy, and spinal compression—but the more operationally disruptive story is increasingly neurological and sensory.
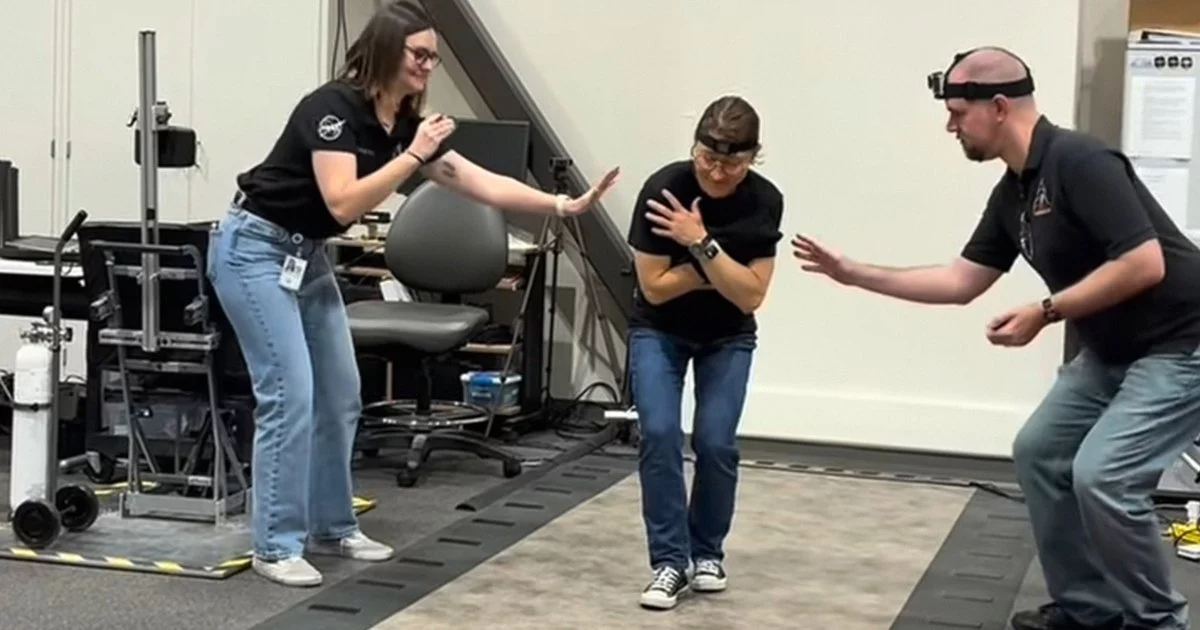
A widely circulated post-flight clip of NASA astronaut Christina Koch struggling to walk a straight line with her eyes closed captures the phenomenon with unusual clarity. It is not simply “weak legs” after a mission. It is the brain returning from an environment where the inner ear’s balance organs (vestibular system) have been functionally downweighted, leaving astronauts over-reliant on vision to stay upright. Remove visual cues, and the newly learned strategy collapses.
For mission planners, this is not a curiosity—it is a readiness issue. For business and technology leaders, it is a market signal: the next wave of space-health innovation will be built around neuroplasticity, sensor fusion, and precision rehabilitation, not just treadmills and resistance bands.
The vestibular reset problem: neuroplasticity across gravity regimes
In microgravity, vestibular hair cells no longer provide reliable head-orientation information. The central nervous system adapts by reweighting inputs—leaning more heavily on proprioception (body position feedback) and vision. That adaptation is beneficial in orbit, but it becomes maladaptive on Earth, where gravity again dominates the physics of balance.
This “gravity transition” exposes a gap in current countermeasures. In-flight exercise can maintain cardiovascular fitness and muscle function, yet it does not fully prevent the sensory recalibration that makes early post-landing mobility uncertain. Today, rehabilitation is often described bluntly: time is the primary cure.
That reliance on time is precisely where technology can intervene. Emerging opportunities point toward a new class of closed-loop vestibular rehabilitation:
- Wearable inertial measurement units (IMUs) to quantify sway, gait asymmetry, and head-motion tolerance in real time
- Haptic feedback systems (vibration cues on the torso or limbs) to substitute for missing vestibular confidence signals
- Augmented reality (AR) overlays that provide dynamic visual anchors and graded balance challenges
- Neural-feedback protocols that train the brain’s sensory weighting more quickly after re-entry
The commercial logic is compelling: the same toolchain that helps astronauts re-adapt could address large terrestrial markets, including vestibular disorders, post-concussion balance deficits, stroke rehabilitation, and fall prevention in older adults. Spaceflight becomes a high-stakes validation environment for technologies that can later scale through clinical pathways on Earth.
Skeletal and spinal countermeasures: from resistive exercise to bioactive interventions
Microgravity accelerates bone loss in ways that resemble osteoporosis—but at a pace that compresses decades of aging into months. Current resistive exercise devices are essential, yet the data continue to suggest a mismatch: muscle can be trained more readily than bone can be preserved. Spinal changes and fluid shifts further complicate the picture, influencing posture, back pain, and potentially ocular outcomes.
This is where next-generation interventions begin to look less like gym equipment and more like bioengineering:
- Osteoinductive growth factor delivery concepts, potentially localized to high-risk skeletal regions
- Electromagnetic or mechanical stimulation approaches aimed at promoting bone remodeling signals
- Improved in-flight diagnostics to detect early skeletal degradation and personalize countermeasures
- Rehabilitation platforms that integrate strength, balance, and neuromotor retraining rather than treating them as separate problems
The strategic significance extends beyond exploration. If space programs can validate faster, more effective bone-preservation methods, the spillover into orthopedics, geriatric medicine, and long-term immobilization care could be substantial. For med-tech firms, “space-qualified” evidence can become a differentiator—particularly if regulators accept spaceflight as an extreme-condition analogue that strengthens safety and efficacy claims.
Space genomics and the actuarial frontier: health risk becomes a data problem
Perhaps the most consequential long-horizon signal is biological: reports of DNA methylation shifts and telomere length alterations during and after missions. The downstream implications remain uncertain, but the direction is clear: spaceflight health risk is moving from visible deconditioning to molecular and epigenetic uncertainty.
That uncertainty changes the economics of human spaceflight. As governments expand Artemis-linked ambitions and private operators scale commercial missions, stakeholders will need clearer answers to questions that are simultaneously medical and financial:
- What biomarkers predict who will experience severe vestibular disruption or prolonged recovery?
- Which genomic or epigenetic signatures correlate with long-term risk?
- How should insurers price coverage when the liability tail is not well characterized?
This is where “space omics” databases and AI-driven pattern recognition become more than research tools—they become infrastructure. A robust, privacy-aware data ecosystem could enable predictive diagnostics and personalized countermeasures, while also informing actuarial models for insurers underwriting crewed missions and space tourism. Expect growing interest in outcome-based contracting in aerospace healthcare, where vendors are paid not only for devices or services, but for measurable reductions in recovery time and complication rates.
The non-obvious spillovers are equally notable. Understanding how the brain leans on visual cues when vestibular inputs are degraded could inform autonomous vehicle passenger comfort algorithms and motion-sickness mitigation in advanced driver-assistance systems. Likewise, astronaut deconditioning research can translate into sports science protocols for balance injuries and concussion recovery, and into workplace ergonomics for partial-gravity habitat design with terrestrial applications in industrial settings.
The Artemis era is making one point unavoidable: the limiting factor for deep-space ambition is not propulsion alone—it is the human operating system. The organizations that can quantify, predict, and shorten the body’s recovery from microgravity will shape not just the safety envelope of lunar and Mars missions, but a broader health-technology market where space is the proving ground and Earth is the scale.
 By
By
 By
By
 By
By

 By
By
 By
By
 By
By
 By
By